A wide variety of calcifications were seen in the head and neck region.
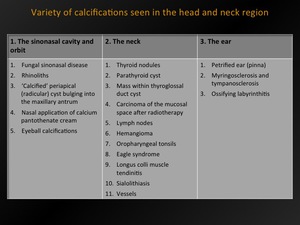
Fig. 1: Variety of calcifications - overview
|
1.
THE SINONASAL CAVITY AND ORBIT
|
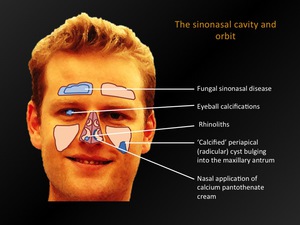
Fig. 2: The sinonasal cavity and orbit - overview
|
1.1.
Fungal sinonasal disease
Invasive versus noninvasive
|
Noninvasive fungal disease
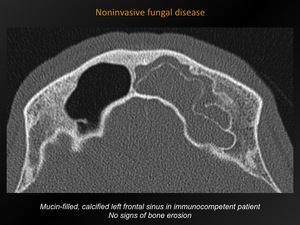
Fig. 3: Noninvasisve fungal disease
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Presence of fungal hyphae within the mucosa of the paranasal sinuses.
Can be acute or chronic.
Symptoms:
Chronic headaches,
nasal congestion,
and chronic sinusitis,
often for years.
CT appearance:
Usually bilateral,
multiple sinuses involved.
High attenuation mucin within lumen of sinuses.
Mostly central calcifications,
with fine/punctate appearance.
Epidemiology/etiology:
Often Aspergillus infection in younger immunocompetent patients,
history of atopy,
asthma or nasal polyps.
Incidence: 6-9% of all rhinosinusitis cases requiring surgery.
Differential Diagnosis:
Nonfungal sinusitis (in which calcifications are rare,
when present mostly peripheral,
round to eggshell appearance)
Invasive fungal disease
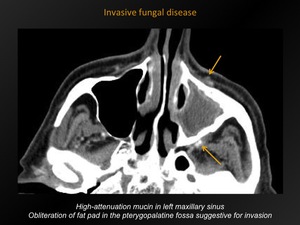
Fig. 4: Invasive fungal disease
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Presence of fungal hyphae within the mucosa,
submucosa,
bone,
or blood vessels of the paranasal sinuses.
Classified as acute or chronic.
Symptoms:
- Acute: fever,
facial pain,
nasal congestion,
changes in vision or mentation,
diplopia.
- Chronic: more indolent,
chronic sinusitis,
few systemic complaints,
visual or neurologic impairment with extensive invasion.
CT appearance:
Mostly unilateral,
high attenuation mucin.
Early: periantral soft tissue infiltration is suspicious for invasion.
Advanced: bone destruction,
intracranial/intraorbital extension.
Epidemiology/etiology:
Often Aspergillus in severe (acute) or moderately (chronic) immunocompromised patients.
Invasive aspergillosis seen in 10-30% of severely immunocompromised patients,
of which 5% have isolated invasive sinusitis.
High mortality.
Differential diagnosis:
Malignancy
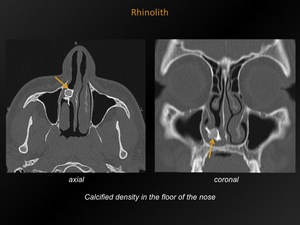
Fig. 5: Rhinolith
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Calcareous concretion formed by deposition of salts on an intranasal foreign body.
Symptoms:
Purulent rhinorrhea and/or ipsilateral nasal obstruction.
CT appearance:
Density usually in the floor of the nose.
Epidemiology/etiology:
Rare condition.
More common in women in third decade,
but can occur at any age.
Presence of a foreign body predisposes to a chronic inflammatory reaction and the precipitation of salts.
Air promotes concentration and crystallization.
Differential Diagnosis:
Fungal disease
|
1.3.
‘Calcified’ periapical (radicular) cyst bulging into the maxillary antrum
|
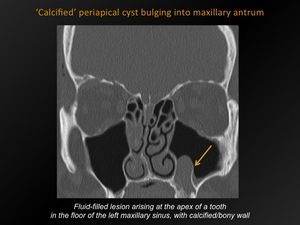
Fig. 6: 'Calcified' periapical cyst bulging into maxillary antrum
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Odontogenic cyst arising at the apex of an infected tooth,
with bony/calcified lining.
Symptoms:
Usually asymptomatic.
CT appearance:
Fluid-containing lesion,
arising at the apex of a tooth,
wih bony/calcified wall.
Epidemiology/etiology:
Odontogenic cystst seen in up to 10% of patients visiting dentist: most often periapical cyst (50%).
More common in men in third to fourth decade.
‘Calcified wall’ not previously described in literature.
Etiology unknown: calcification in wall or bone erosion?
Differential Diagnosis:
Retention cyst,
any other maxillary cyst
|
1.4.
Nasal application of calcium pantothenate cream
|
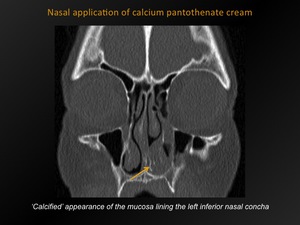
Fig. 7: Nasal application of calcium pantothenate cream
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Dense appearance of the mucosa lining the septum and inferior nasal concha due to calcium in cream.
Symptoms:
History of nose bleeds,
dry mucosa treated with calcium pantothenate cream.
CT appearance:
‘Calcified’ appearance of the mucosa lining the septum and inferior nasal concha.
Epidemiology/etiology:
No numbers reported in literature.
Cream applied to nose contains calcium,
explaining the dense appearance on CT.
Differential Diagnosis
Fungal disease,
rhinolith
|
1.5.
Eyeball calcifications
|
A wide variety of eyeball and orbital calcifications is noted on CT exams (orbital calcifications are seen in 8% of the population).
Most are of no clinical significance.
In children,
eyeball calcifications should always alert the radiologist for the presence of a retinoblastoma.
Optic nerve drusen
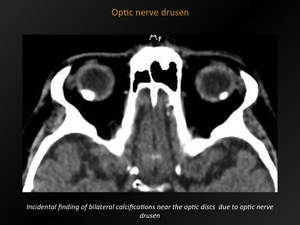
Fig. 8: Optic nerve drusen
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Calcifications at the optic nerve head.
Symptoms:
Often asymptomatic,
‘pseudo’papilledema on ophtalmoscopic inspection.
May be associated with visual field defects.
CT appearance:
Punctate calcifications seen near the optic disc on cross-sectional images.
Epidemiology:
Typically seen in patients with age-related macular degeneration (but even described in children).
Occurs in 3,4-24/1000 patients.
Bilateral in 75%.
Differential Diagnosis:
In children: retinoblastoma until proven otherwise.
Retinoblastoma
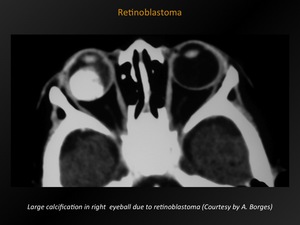
Fig. 9: Retinoblastoma
References: A. Borges; Lisboa, PORTUGAL
Definition:
Malignant intra-ocular tumor in childhood.
Symptoms:
Leukocoria,
strabismus,
vision loss.
CT appearance:
Typical appearance: enhancing mass with calcifications of different number,
size and shape.
In case of optic nerve involvement: thickened appearance of the optic nerve.
In more advanced cases: large mass extending into retro-orbital soft tissue,
extra-orbital or intracranial tissues.
Epidemiology:
Most common intra-ocular tumor in children (3% of all cancers < 15 years).
More than 95% of all cases are diagnosed before the age of 5 years.
Foci of calcification are present in 90% of all retinoblastoma cases.
Differential Diagnosis:
Optic nerve drusen,
microphtalmos,
retinal astrocytoma,
retinopathy of prematurity,
cytomegaly retinitis,
toxocariasis and medulloepithelioma

Fig. 10: The neck - overview
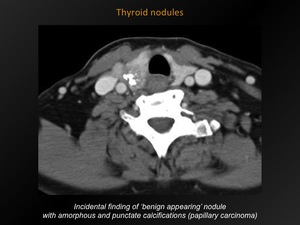
Fig. 11: Thyroid nodules
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Nodule in thyroid gland containing calcium.
Symptoms:
Often asymptomatic.
When large: symptoms of tracheal compression.
CT appearance:
No CT feature reliably distinguishes benign from malignant lesions.
Punctate,
linear,
eggshell,
amorphous or nodular calcifications occur in both benign and malignant thyroid tumors.
Fine,
punctate calcifications are suspect for malignancy (papillary > medullary carcinoma).
Epidemiology:
Thyroid nodules are extremely common: clinically apparent nodules are seen in 6,5% of women and 1,5% of men.
Incidental thyroid lesions are detected with CT in 15% of the cases,
of which 10% are malignant (especially in patients <35 years).
Punctate calcifications occur in ca.
12% of incidentally detected lesions.
Differential Diagnosis:
Appearance typical enough to make a confident diagnosis as such.
|
2.2.
Calcified parathyroid cyst
|
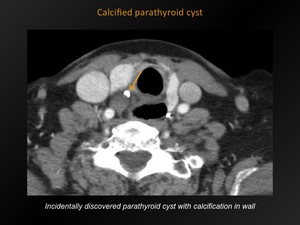
Fig. 12: Calcified parathyroid cyst
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Cystic lesion in the region of the parathyroid gland as a result of degeneration of parathyroid adenoma or embryologic remnants of pharyngeal pouches.
Symptoms:
Usually asymptomatic.
When large: symptoms of tracheal or esophageal compression.
CT appearance:
Hypodense,
sharply delineated mass in the region of the parathyroid.
Calcification is very rare.
Epidemiology:
Rare: 0,6% of all thyroid and parathyroid lesions.
Mostly nonfunctioning cysts: more common in women,
mean age 43,3 years.
Functioning cysts (11-30%): more common in men,
mean age 51,9 years.
Differential Diagnosis:
Parathyroid adenoma or carcinoma,
thyroid or thymic cyst,
necrotic lymph node
|
2.3.
Mass within thyroglossal duct cyst
|
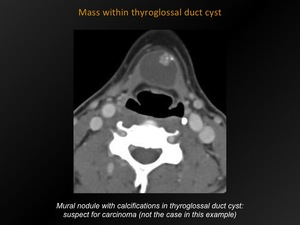
Fig. 13: Mass within thyroglossal duct cyst
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Presence of a mass within the midline,
cystic remnant of the embryologic thryoglossal duct.
Symptoms:
Presence of an anterior neck mass.
CT appearance:
Benign cyst: midline,fluid-attenuated mass near the level of the hyoid bone,
with a thin,
smooth wall.
Calcification and/or dense or enhancing mural nodules: suspect for carcinoma.
Epidemiology:
Congenital lesion,
50% discovered after age of 10 years.
Most common congenital cyst: 90% of all congenital neck abnormalities.
Development of carcinoma in 1% of thyroglossal duct cysts (mostly papillary Ca)
Differential Diagnosis:
Dermoid/sebaceous cyst,
branchial cleft cyst,
lymph node,
lymphatic malformation
|
2.4.
Carcinoma of the mucosal space after radiotherapy
|
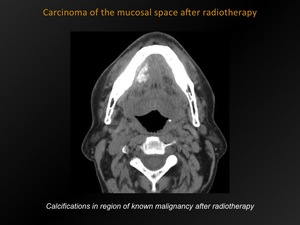
Fig. 14: Carcinoma of the mucosal space after radiotherapy
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Carcinoma in the superficial layer of the oral cavity and pharynx containing calcium after radiotherapy.
Symptoms:
No specific symptoms.
CT appearance:
Irregular calcifications appearing in the mucosal space,
in the region of the known malignancy .
Epidemiology:
Dystrophic calcification as a result of radiotherapy well-known and frequent elsewhere in the body.
No exact numbers in literature concerning frequency in the head and neck (rare to our experience).
Differential Diagnosis:
Usually preoperative imaging present: differential diagnosis not difficult.
|
2.5.
Cervical lymph node calcification
|
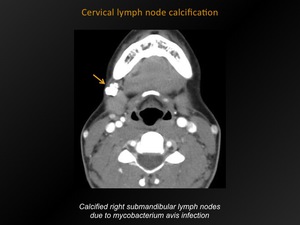
Fig. 15: Cervical lymph node calcification
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Presence of calcium in one or morecervical lymph nodes.
Symptoms:
None,
sometimes neck mass.
CT appearance:
Calcification in one or more of the cervical nodal regions.
Epidemiology:
Cervical nodal calcification is seen in 1% of CT scans.
Differential Diagnosis:
Tuberculosis,
treated lymphoma,
metastatic thyroid carcinoma,
adenocarcinoma or squamous cell carcinoma and less commonly sarcoidosis,
amyloidosis,
treated acute infection,
...
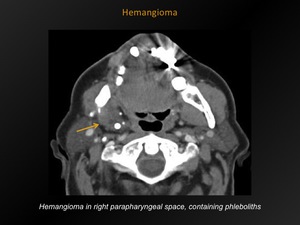
Fig. 16: Hemangioma
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Benign vascular malformation.
Three types: capillary,
cavernous,
or mixed type.
Symptoms:
Often asymptomatic.
When large enough: neck mass.
When superficial: bluish color of the skin/mucosa.
CT appearance:
Hypodense mass relative to muscle containing dense phleboliths.
If serial imaging is performed after IV injection of a iodinated contrast agent,
increasing enhancement is noted over time.
Epidemiology:
Congenital,
rapid growth in infancy,
followed by slow regression.
Most common head and neck tumor in infancy: occurs in ca.
5% of all children (mostly females).
Predilection for the head and neck region.
Differential Diagnosis:
Mainly lymphangioma.
Any other well defined mass (branchial cleft cyst,
schwannoma,
…).
|
2.7.
Calcified oropharyngeal tonsils
|
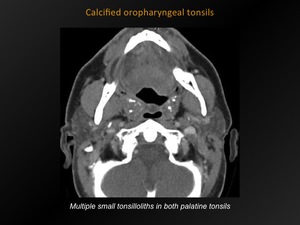
Fig. 17: Calcified oropharyngeal tonsils
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Synonym ‘tonsilloliths’.
Small areas of calcareous matter formed in the tonsillar crypts.
Symptoms:
Asymptomatic or throat irritation,
foul taste and odor,
otalgia.
CT appearance:
Multiple,
clustered,
ovoid homogeneous densities located in the oropharyngeal tonsils.
Epidemiology:
Relatively frequent (no exact numbers reported in literature).
Mostly in palatine tonsils,
might occur in lingual tonsils.
Differential Diagnosis:
Appearance typical enough to make a confident diagnosis as such.
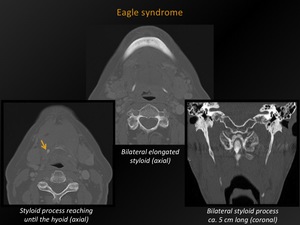
Fig. 18: Eagle syndrome
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Variety of symptoms caused by elongated ossified styloid process or calcified stylohyoid ligament.
Symptoms:
Dysphagia,
headache,
painful neck rotation,
painful extension of the tongue,
change in voice,
sensation of hypersalivation.
CT appearance:
Length styloid process > 3 cm (this is the average of different measurements noted in literature and roughly varying between 2,5-4 cm).
Epidemiology:
Elongated styloid process occurs in 4% of the population.
Only 4-10% is symptomatic (this syndrome has believers and non-believers).
Differential Diagnosis:
Appearance typical enough to make a confident diagnosis as such.
|
2.9.
Longus colli muscle tendinitis
|
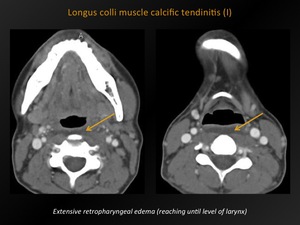
Fig. 19: Longus colli muscle calcific tendinitis (I)
References: M. Lemmerling; Beervelde, BELGIUM
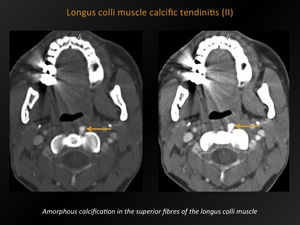
Fig. 20: Longus colli muscle calcific tendinitis (II)
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Retropharyngeal inflammatory process of the longus colli muscle tendon.
Symptoms:
Acute onset of neck pain and stiffness,
odynophagia,
dysphagia.
CT appearance:
Variable degree of amorphous calcification,
typically in the superior fibres of the longus colli muscle tendons (C1-C2 level).
Accompanying retropharyngeal effusion.
Epidemiology:
Rare,
no exact numbers reported in literature.
Patients 20-80 years old,
typically patients in sixth decade.
Differential Diagnosis:
Suppurative retropharyngeal infection,
fracture dislocation of the cervical spine,
myositis ossificans,
primary or metastatic neoplasia.
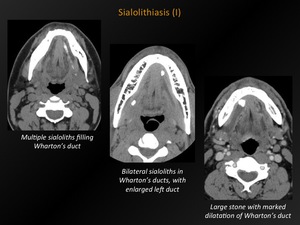
Fig. 21: Sialolithiasis (I)
References: M. Lemmerling; Beervelde, BELGIUM
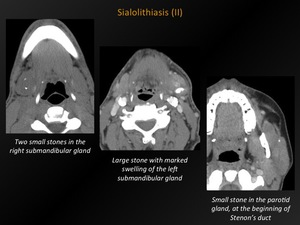
Fig. 22: Sialolithiasis (II)
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Calculi formed in the salivary glands or ducts.
Symptoms:
Depending on location: when in gland itself,
symptoms may be minor.
Ductal sialoliths more often cause symptoms: pain and swelling of the gland.
CT appearance:
Solitary or multiple calcifications in the salivary glands.
When obstructive: swelling of the salivary gland and/or dilatation of the salivary duct,
filled with hypodense saliva.
Epidemiology:
Second most common disease of the salivary glands after mumps.
80-90% of sialoliths occur in the submandibular gland,
10-20% in the parotid glands and 1-7% in the sublingual gland.
Solitary sialolith in 75%,
multiple in 25%.
Bilateral stones are rare (2%).
Differential Diagnosis:
After intravenous injection of contrast: small opacified blood vessel may simulate sialoliths (CT best initially without contrast).

Fig. 23: Vessels
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Calcifications present in carotid artery plaque.
Symptoms:
Often asymptomatic.
May lead to transient ischemic attack or stroke.
CT appearance:
Calcifications in the vessel wall of the common carotid artery,
the carotid bifurcation,
the internal (and external) carotid artery,
with or without significant plaque stenosis.
Epidemiology:
Strong association between carotid artery calcification and stroke (OR 4).
Stroke incidence >55years: 4,2-11,7/1000/year (61-81% ischemic).
Age-standardised stroke prevalence rate >65years: 46-73/1000.
More than half of all strokes occur in people over 75 years.
One-month case-fatality for ischemic stroke is 16%.
Differential Diagnosis:
Appearance typical enough to make a confident diagnosis as such.
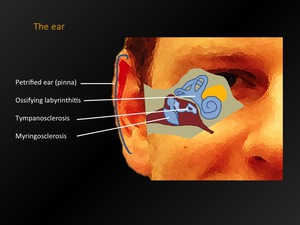
Fig. 24: The ear - overview
|
3.1.
Petrified ear (pinna)
|
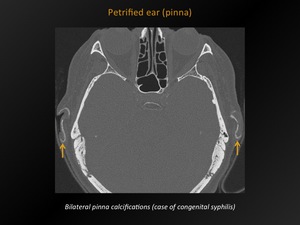
Fig. 25: Petrified ear (pinna)
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Calcification or new bone formation along the cartilage of the auricle.
Symptoms:
Asymptomatic.
Sometimes discomfort when pressure to ears is applied.
CT appearance:
Hyperdense areas along the auricles (localised or diffuse).
Epidemiology/etiology::
Rare (examination of 800 patients aged 15-75years: no one with auricular rigidity.
Other study found radiological auricular calcification in 3% of the cases,
but each of these patients had diseases known to cause ectopic calcification such as acromegaly,
scleroderma and diabetes mellitus).
Differential Diagnosis:
Appearance typical enough to make a confident diagnosis as such.
|
3.2.
Myringosclerosis and tympanosclerosis
|
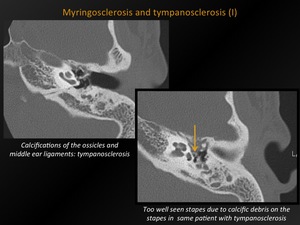
Fig. 26: Myringosclerosis and tympanosclerosis (I)
References: M. Lemmerling; Beervelde, BELGIUM

Fig. 27: Myringosclerosis and tympanosclerosis (II)
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Deposition of calcium in the tympanic cavity.
Symptoms:
Hearing loss,
mostly conductive type (sometimes mixed).
CT appearance:
Solitary or multifocal punctate,
web-like calcifications in the middle ear cavity or on the tympanic membrane.
May be in direct apposition to the ossicular chain or the suspensory ligaments of the ossicles.
Different terminologies:
-Myringosclerosis: calcifications isolated to the tympanic membrane.
-Tympanosclerosis: also calcifications on the ossicles and middle ear ligaments and muscle tendons.
Epidemiology:
Incidence 11,6% in chronic suppurative otitis media patients.
85,6% of tympanosclerosis patients have dry ear.
Differential Diagnosis:
Appearance typical enough to make a confident diagnosis as such.
|
3.3.
Ossifying labyrinthitis
|
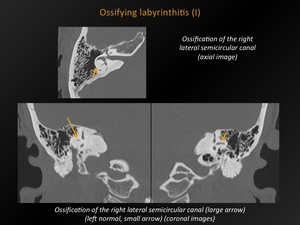
Fig. 28: Ossifying labyrinthitis (I)
References: M. Lemmerling; Beervelde, BELGIUM
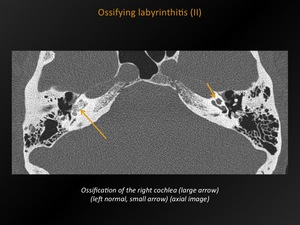
Fig. 29: Ossifying labyrinthitis (II)
References: M. Lemmerling; Beervelde, BELGIUM
Definition:
Pathologic calcification/formation of new bone within the lumen of the otic capsule.
Symptoms:
Sensorineural hearing loss and loss of vestibular function.
CT appearance:
Calcification/ossification in the cochlea,
the vestibule or the semicircular canals.
Epidemiology/etiology:
Mostly results from purulent labyrinthitis caused by bacterial meningitis (meningogenic type) or otitis media (tympanogenic type),
respectively bilateral and unilateral.
Other causes: septic emboli,
cholesteatoma,
etc.
After meningitis,
profound deafness occurs in 5% of patients: 80% of these patients have labyrinthine ossification.
Differential Diagnosis:
Labyrinthine hypogenesis or agenesis



















 References: M. Lemmerling; Beervelde, BELGIUM")
 References: M. Lemmerling; Beervelde, BELGIUM")
 References: M. Lemmerling; Beervelde, BELGIUM")
 References: M. Lemmerling; Beervelde, BELGIUM")


 References: M. Lemmerling; Beervelde, BELGIUM")
 References: M. Lemmerling; Beervelde, BELGIUM")
 References: M. Lemmerling; Beervelde, BELGIUM")
 References: M. Lemmerling; Beervelde, BELGIUM")
 References: M. Lemmerling; Beervelde, BELGIUM")